Rare diseases refer to a group of diseases with a low prevalence rate, but collectively, they affect a significant percentage of the world population. However, their low prevalence poses a challenge for research as there is limited access to biological samples and patient databases. This leads to insufficient medical expertise and inadequate care for patients with rare diseases. The majority of rare diseases are genetic, with muscular dystrophies being an important class. Although rare diseases present a challenge for drug development, monoclonal antibody-based products are becoming increasingly popular among orphan drugs due to their high therapeutic efficacy in targeting specific molecule functions and signaling pathways in rare cancers and autoimmune diseases. However, these products come with a high production and acquisition cost, resulting in a significant economic burden for both patients and society.
A Breakthrough Treatment for Paroxysmal Nocturnal Hemoglobinuria (PNH)
The complement system is important for the immune system, but if it becomes overactive, it can lead to serious health problems. Paroxysmal nocturnal hemoglobinuria (PNH) is a rare blood disorder caused by genetic mutations that lead to a deficiency of certain surface proteins on blood cells, including CD59, which inhibits the complement system. This results in chronic intravascular hemolysis, a process that causes many of the symptoms of PNH. Eculizumab, a humanized monoclonal antibody that targets complement component C5, has been developed and approved as a treatment for PNH. It blocks the harmful effects of terminal complement activation and is an effective therapy for PNH.
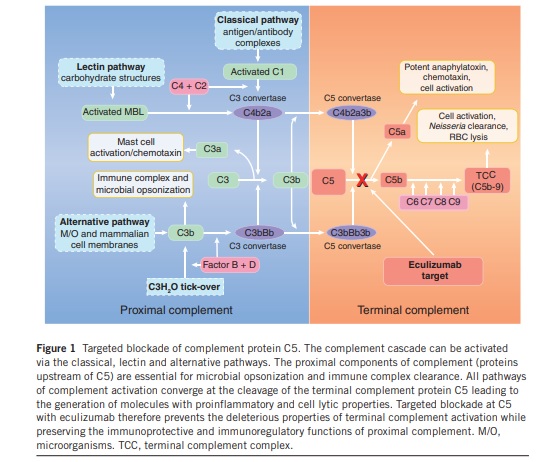
Eculizumab targeting complement component C5, blocks the terminal complement activation in PNH treatment.
All the pathways of complement activation converge at the C5 cleavage into C5a and C5b by C5 convertase enzymes, which initiates the terminal complement cascade. C5a is a potent anaphylatoxin that induces secondary inflammatory mediators, such as cytokines, reactive oxygen species, hydrolytic enzymes, and arachidonic acid metabolites, alters smooth muscle tone, increases vascular permeability, and mediates leukocyte chemotaxis. C5a receptors are present in several cell types that contribute to inflammation, such as monocytes, macrophages, and neutrophils. C5b recruits the terminal complement components C6, C7, C8, and C9 to form the TCC on cell surfaces. The generation of TCC (Terminal complement complex) at sublytic concentrations leads to the release of many of the same proinflammatory molecules as C5a and the unimpeded assembly of TCC on the cell surface results in cell lysis. In hemolytic diseases such TCC deposition on erythrocytes leads to their destruction.
The Role of Precision Medicine and Eculizumab’s Modified Antibody
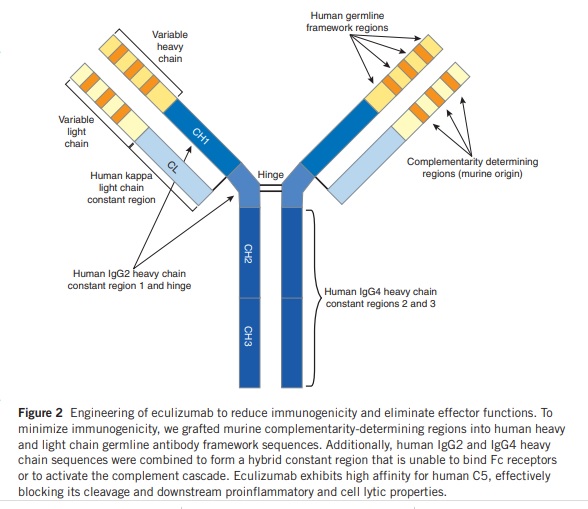
Eculizumab is an example of precision medicine because it is specifically designed to target a particular molecule that is involved in the development and progression of certain diseases. Precision medicine involves using a patient’s genetic and other biological information to tailor medical treatment to their individual needs. The humanized antibody was designed to minimize immunogenicity by using complementarity-determining regions from m5G1.1 and germline-based frameworks. The heavy-chain constant region was replaced with components from human IgG2 and IgG4 to reduce proinflammatory responses. The resulting hybrid constant region lacks the ability to bind Fc receptors or activate complement, and a common cleavage site was used to avoid generating an antigenic site.
Eculizumab: Clinical development and potential use in other rare diseases
Eculizumab underwent a decade of clinical development before its approval for the rare and life-threatening blood disorder PNH. Prior to its use in PNH, the drug’s safety profile and immunomodulatory effects were assessed through studies. The PNH clinical program was extensive, involving multinational trials with 195 participants, and allowing for careful evaluation of both biochemical and clinically validated measurements. This approach can be used to consider eculizumab in other rare and life-threatening diseases where there is evidence of terminal complement involvement, such as lupus, myasthenia gravis, and multiple sclerosis. The understanding of eculizumab’s pharmacokinetic and pharmacodynamic properties in PNH patients and large-scale commercial manufacturing has also made it possible to evaluate new formulations of the drug for other diseases, including age-related macular degeneration and asthma.
Precision Medicine in Rare Diseases: A Focus on Antibody-Based Therapies
Antibody-based therapies have emerged as a promising approach for the treatment of rare diseases. However, the effector functions of antibodies, such as complement activation and Fc receptor binding, can lead to proinflammatory responses and other complications. To address these challenges, precision medicine approaches are needed to develop antibody therapies with modified constant regions that retain antigen specificity but reduce effector function. This requires a deep understanding of the molecular mechanisms underlying rare diseases, as well as careful consideration of the unique features of each patient population. Nevertheless, precision medicine approaches have the potential to transform the treatment of rare diseases by enabling the development of more effective and targeted therapies that minimize adverse effects and improve patient outcomes.
High cost: The cost of PM and antibody therapies can be very high, making them inaccessible to many patients. For example, CAR-T cell therapy, a type of immunotherapy, can cost over $500,000 per treatment.
Limited applicability: Some PM and antibody therapies are only effective in a subset of patients based on their genetic or molecular profiles, meaning they may not be useful for all patients. For example, the drug vemurafenib is only effective in patients with a specific genetic mutation found in certain types of melanoma.
Development challenges: Developing PM and antibody therapies can be challenging and time-consuming, as the therapies need to be tailored to specific molecular targets. This can also lead to challenges in obtaining regulatory approval for these therapies. For example, it took several years for the first CAR-T cell therapy to be approved by the FDA.
Potential side effects: PM and antibody therapies can have significant side effects, including immune-related adverse events. For example, checkpoint inhibitors, a type of immunotherapy, can cause autoimmune disorders such as colitis or thyroiditis.
Resistance: Some patients may develop resistance to PM and antibody therapies over time, leading to the therapy becoming ineffective. For example, patients with chronic myeloid leukemia may develop resistance to the drug imatinib, which targets a specific molecular target.
Case studies of advancing precision medicine with antibody-based therapies for rare diseases
Here are a few case studies of how antibody-based therapies are being used to advance precision medicine for rare diseases:
Spinal muscular atrophy (SMA): SMA is a rare genetic disorder that affects the nervous system and leads to muscle wasting and weakness. In 2016, the FDA approved nusinersen, a monoclonal antibody therapy, for the treatment of SMA. Nusinersen works by targeting the genetic cause of the disease and has shown to significantly improve motor function and increase survival in patients with SMA.
Pompe disease: Pompe disease is a rare genetic disorder that affects the muscles and leads to progressive weakness and respiratory failure. In 2014, the FDA approved alglucosidase alfa, a monoclonal antibody therapy. Alglucosidase alfa works by replacing the missing enzyme in patients with Pompe disease and has shown to improve respiratory function and quality of life.
Gaucher disease: Gaucher disease is a rare genetic disorder that affects the liver, spleen, and bone marrow. In 2006, the FDA approved imiglucerase for the treatment of Gaucher disease. Imiglucerase works by replacing the missing enzyme in patients with Gaucher disease and has shown to improve hematologic and visceral parameters.
These case studies demonstrate the potential of antibody-based therapies to address the underlying genetic causes of rare diseases and improve patient outcomes. By targeting specific molecular pathways and mechanisms, these therapies offer a more precise and personalized approach to treatment.
Precision Medicine and Monoclonal Antibodies: Advancing Care for Patients with Rare Diseases
Precision medicine has the potential to transform the treatment of rare diseases with monoclonal antibody therapies. However, achieving this potential will require increased investment and collaboration among researchers, industry, healthcare providers, patient organizations, and policymakers.
To advance precision medicine for rare diseases, there is a need to improve our understanding of the underlying biology and genetic mechanisms of these diseases and to develop better tools and technologies for diagnosing and monitoring them. This will require sustained funding for research, as well as partnerships between academic institutions, industry, and patient groups.
In addition, regulatory agencies must continue to adapt to the changing landscape of precision medicine and support the development of innovative monoclonal antibody therapies for rare diseases. This includes providing expedited approval pathways for these therapies and ensuring that reimbursement policies are aligned with the value they provide.
Ultimately, the success of precision medicine for rare diseases will depend on the ability of all stakeholders to work together towards common goals. By pooling our resources and expertise, we can accelerate the development of new therapies and improve the lives of patients with rare diseases.
References
- Guiraud, S.; Aartsma-Rus, A.; Vieira, N.M.; Davies, K.E.; van Ommen, G.J.; Kunkel, L.M. The pathogenesis and therapy of muscular dystrophies. Annu. Rev. Genomics Hum. Genet. 2015, 16, 281–308. [CrossRef] [PubMed].
- Stavrou, M.; Sargiannidou, I.; Georgiou, E.; Kagiava, A.; Kleopa, K.A. Emerging therapies for Charcot-Marie-Tooth inherited neuropathies. Int. J. Mol. Sci. 2021, 22, 6048.
- Rother, R., Rollins, S., Mojcik, C. et al. Discovery and development of the complement inhibitor eculizumab for the treatment of paroxysmal nocturnal hemoglobinuria. Nat Biotechnol 25, 1256–1264 (2007). https://doi.org/10.1038/nbt1344.
- Mueller, J.P. et al. Humanized porcine VCAM-specific monoclonal antibodies with
Chimeric IgG2/G4 constant regions block human leukocyte binding to porcine endothelial cells. Mol. Immunol. 34, 441–452 (1997).
- . Canfield, S.M. & Morrison, S.L. The binding affinity of human IgG for its high-affinity Fc receptor is determined by multiple amino acids in the CH2 domain and is modulated by the hinge region. J. Exp. Med. 173, 1483–1491 (1991).
- Burton, D.R. & Woof, J.M. Human antibody effector function. Adv. Immunol. 51, 1–84 (1992).
- Breedveld FC. Therapeutic monoclonal antibodies. Lancet. 2000; 355(9205):735–40.