Personalized medicine involves customizing medical treatment for individual patients based on their genetic and disease-related factors. By utilizing genomic and transcriptomic information, this approach can provide more effective treatments and reduce medical costs. In the preclinical stage, individuals may not exhibit any symptoms but may show biomarker changes associated with the disease. Mild cognitive impairment is characterized by noticeable cognitive decline but without significant impairment in activities of daily living.
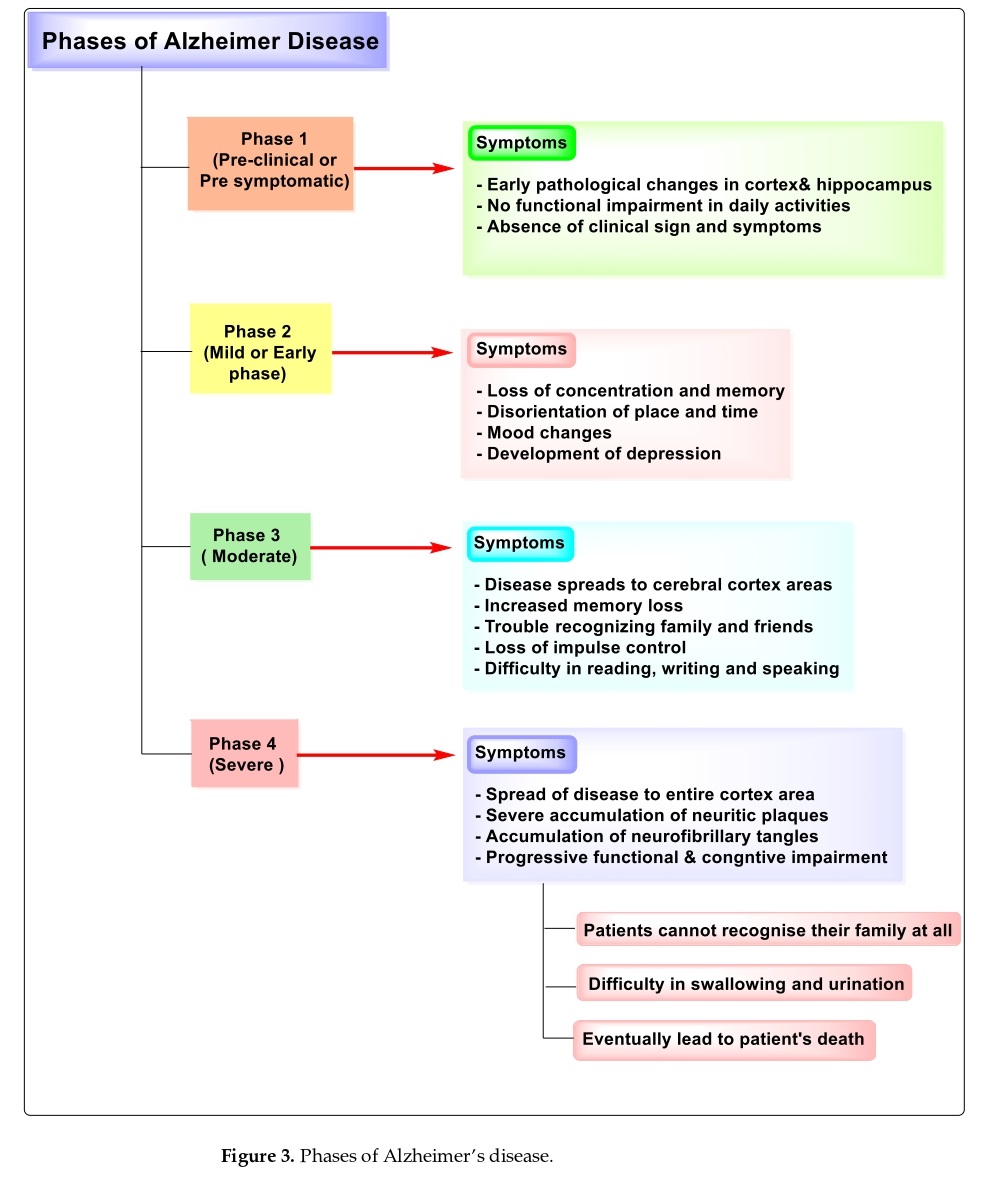
Stages of Alzheimer’s disease
The mild or early stage involves loss of focus and memory, disorientation, mood swings, and depression. The moderate stage expands to a portion of the cerebral cortex causing memory loss, difficulty acknowledging people, impulse control loss, and difficulties in speaking, reading, and writing. The severe stage expands to the entire cortex leading to cognitive and functional impairment, an inability to recognize family members, and difficulties in urination and swallowing resulting in death.
A brief overview of Alzheimer’s disease and its current treatment options
The formation of Ab peptides and small oligomers is thought to be a key factor in the development of the disease. Preventing or reversing the formation of amyloid is considered a promising strategy for AD treatment. This has led to the development of various therapeutic approaches, including active and passive immunization against Ab peptides. These approaches have shown promising results in preclinical studies and clinical trials, leading to the initiation of several ongoing trials using immunization approaches.
Vaccination with Ab1-42 in AD transgenic mice resulted in reductions in plaque deposition and cognitive improvement. However, clinical trials of aggregated Ab vaccination (AN1792) had to be terminated due to meningoencephalitis induced by T-cell-mediated and/or Fc-mediated immune responses. New vaccination strategies and direct administration of human/humanized monoclonal/polyclonal antibodies against Ab are being explored as potential treatment options to circumvent unwanted T-cell responses.
Antibody Therapy for Alzheimer’s Disease
Central region-specific antibodies increase the level of plasma Ab and accelerate the Ab efflux from the brain to the blood plasma, thereby providing a ‘peripheral sink’ for Ab clearance. C-terminal region-specific antibodies reduce brain Ab levels and protect hippocampal neurons against oxidative stress. New antibody formats have been developed that recognize specific conformational epitopes and bind to aggregated Ab such as protofibrils, oligomers, or amyloid plaques but not to monomeric Ab or Ab precursor proteins. These antibodies prevent/reverse the disruption of hippocampal long-term potentiation mediated by Ab oligomers. However, further research is needed to determine the optimal timing and dosing of these therapies for the treatment of Alzheimer’s disease.
Bapineuzumab and Solanezumab: Clinical Trials and Results
Bapineuzumab and solanezumab, humanized monoclonal antibodies, have been tested for passive immunization in large-scale phase-three clinical trials for Alzheimer’s disease (AD) patients. However, many of these trials did not achieve their intended goals. Bapineuzumab targets the N-terminus of amyloid beta and can cause adverse effects like vasogenic edema, especially in APOE e4 (apolipoprotein E epsilon 4) carriers. In a phase 2 trial, it was shown to reduce amyloid beta burden in the brain, but there was no significant difference in CSF (Cerebrospinal fluid) amyloid beta levels between the treatment and placebo groups. However, there was a slight difference in CSF tau protein levels. Large phase-three trials on bapineuzumab have been discontinued due to the lack of clinical benefits. Two ongoing phases 1 clinical trials are testing a re-engineered version of bapineuzumab (AAB-003) for safety and tolerability in mild-to-moderate AD patients, aimed at reducing the risk of adverse effects like ARIAs.
The Economic Impact of Alzheimer’s Disease and the Need for Novel Approaches
Alzheimer’s Disease (AD) is a costly disease that has a significant impact on healthcare systems and society, resulting in both direct and indirect expenses. At present, AD affects about 35 million people worldwide, and this number is expected to reach 115 million by 2050. The costs associated with AD are projected to be approximately 215 billion US dollars, and this is expected to rise to around 500 billion US dollars each year by 2040. The dependence model provides a comprehensive assessment of AD’s progression and its impact on patients and their families. To address the high costs, novel preventive, diagnostic, and therapeutic approaches are needed. Passive amyloid-beta immunotherapy shows promise, despite the challenges posed by its injectable form of delivery. Patients and caregivers can be motivated to adhere to this treatment, particularly those with early-stage AD, with clear communication, education, and support. The Alzheimer’s Disease Education and Referral Center is a dependable source of accurate information on AD, including new treatments and diagnostic tools.
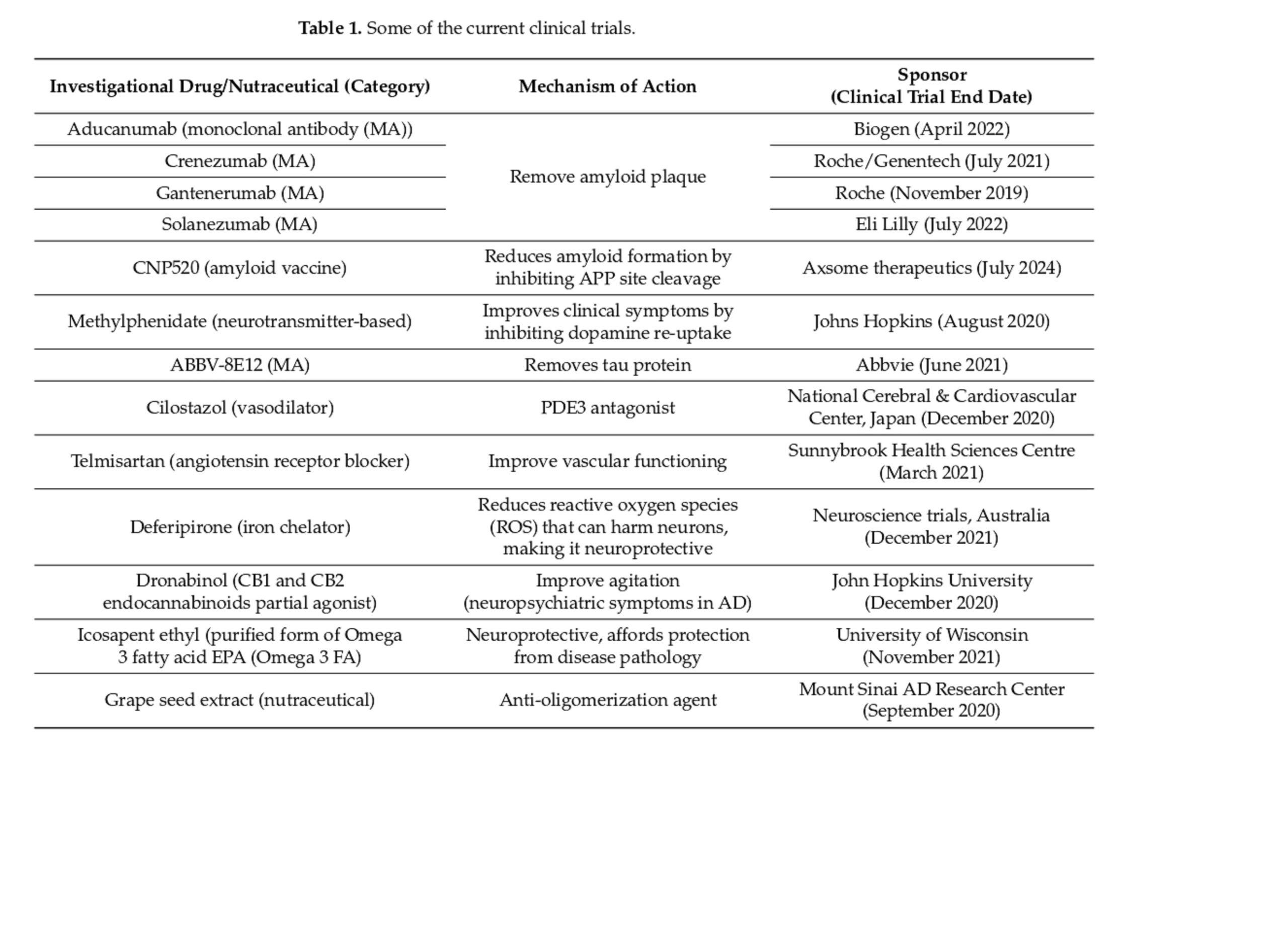
Clinical trials for the treatment of chronic progressive illnesses with multiple medications
Clinical trials are underway to find effective treatments for chronic progressive illnesses, and it’s been observed that using multiple medications that affect multiple receptor targets, can be helpful. The table below lists some examples of drugs that are currently undergoing clinical trials.
The potential of precision medicine and personalized treatments for Alzheimer’s disease
Precision medicine and personalized treatments for Alzheimer’s disease have the potential to identify high-risk patients, detect the disease early, and optimize treatment strategies while minimizing adverse effects. Research has identified several genetic risk factors and lifestyle habits that influence disease susceptibility. Advances in genomic, transcriptomic, and proteomic technologies have enabled the identification of common and rare risk alleles with greater sensitivity and accuracy. Biomarkers and genetic profiles can be used to tailor treatments to individual patients and address specific disease mechanisms.
However, challenges such as the need for accurate biomarkers and standardized diagnostic criteria must be addressed. A better understanding of the complex mechanisms of Alzheimer’s disease is also necessary for developing effective targeted therapies.
The traditional approach does not consider the variability in disease susceptibility and treatment response among individuals or subgroups. Chronic diseases such as cancer, cardiovascular disorders, and dementia have become significant health challenges over the past few decades, and it has been established that a one-size-fits-all treatment approach may not be effective for these multifactorial diseases. Instead, a combination of therapies targeting multiple pathogenic pathways is required for effective treatment.
Soon, clinicians may be able to identify specific predisposing risk alleles in young asymptomatic adults and diagnose the disease pre-symptomatically using biomarkers. Therapeutic approaches could be tailored based on genetic background and biomarker profile, such as administering amyloid-targeting therapies to AD patients before symptoms manifest or using tau therapeutics in combination with Aβ drugs at symptomatic stages.
Clinical trials could be designed based on genetic predisposition and disease stage for better stratification of patients, and a range of biomarker assays could help determine the efficacy of drugs tested in clinical trials more rapidly. Overall, the field of AD is moving towards precision medicine, which has the potential to significantly improve disease diagnosis, treatment, and prevention.
Precision medicine and personalized approaches for neurodegenerative disorders
Recently, it’s been suggested that precision medicine could also be applied to neurodegenerative disorders, using tailored biomarker-guided therapies and personalized approaches based on individual patient characteristics. This approach is necessary due to the many clinical trial failures reported. In the early stages of Alzheimer’s disease, various molecular mechanisms can contribute to its development, and a subject’s profile can be determined by assessing various parameters, including biomarkers and genetic profiles. Systems biology approaches may be useful to obtain a comprehensive understanding of these parameters. By using these approaches, it may be possible to develop effective pharmacological treatments that can address the various pathophysiological profiles seen in neurodegenerative disorders.
Antibody-based therapy for Alzheimer’s disease and its role in precision medicine
Antibody-based therapy has shown potential for treating Alzheimer’s disease, as it targets the accumulation of amyloid-beta plaques, a hallmark of the disease. Monoclonal antibodies such as aducanumab have shown promise in clinical trials, leading to FDA approval for their use in patients with early-stage Alzheimer’s. Other antibody-based therapies are also being developed, including passive immunotherapy and immunization approaches. The use of these therapies in precision medicine for Alzheimer’s disease is promising, as they can be tailored to individual patients based on their biomarker profiles and disease progression. Precision medicine approaches can also help identify patients who are most likely to benefit from antibody-based therapy and optimize treatment strategies. Therefore, antibody-based therapy holds great potential for the future of precision medicine in the treatment of Alzheimer’s disease.
Amyloid-related imaging abnormalities (ARIAs) in clinical trials of monoclonal antibodies for Alzheimer’s disease
During clinical trials of monoclonal antibodies (mAbs) for Alzheimer’s disease, amyloid-related imaging abnormalities (ARIAs) have been observed, which include signal hyperintensities and signal hypo intensities on magnetic resonance imaging (MRI). These abnormalities are thought to be caused by increased vascular permeability due to vascular amyloid deposition. In one study, vasogenic edema (ARIA-E) was observed in treated patients, particularly in those carrying the apolipoprotein E ε4 (ApoE4) gene, and this side effect led to the highest dose not being tested in phase 3 studies. However, ARIAs have not been observed in patients treated with other mAbs. The incidence of ARIA-E in a phase 3 study of solanezumab was not statistically significant.
References
- Brody DL, Holtzman DM. Active and passive immunotherapy for neurodegenerative disorders. Annu Rev Neurosci 2008; 31:175-93.
- Pul, R., Dodel, R., & Stangel, M. (2011). Antibody-based therapy in Alzheimer’s disease. Expert opinion on biological therapy, 11(3), 343-357.
- Sperling RA, Jack CR, Jr, Black SE, Frosch MP, Greenberg SM, Hyman BT, et al. Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: Recommendations from the Alzheimer’s Association Research Roundtable Workgroup. Alzheimer’s Dement. 2011; 7:367–85.
- Lemere CA. Immunotherapy for Alzheimer’s disease: Hoops and hurdles. Mol Neurodegener. 2013; 8:36.
- Rygiel K. Novel strategies for Alzheimer’s disease treatment: An overview of anti-amyloid beta monoclonal antibodies. Indian J Pharmacol. 2016 Nov-Dec; 48(6):629-636. Doi: 10.4103/0253-7613.194867. PMID: 28066098; PMCID: PMC5155461.
- Armstrong, R.A. Risk factors for Alzheimer’s disease. Folia Neuropathol. 2019, 57, 87–105.
- Forloni G. Alzheimer’s disease: from basic science to precision medicine approach. BMJ Neurol Open. 2020 Nov 12;2(2):e000079. Doi: 10.1136/bmjno-2020-000079. PMID: 33681801; PMCID: PMC7903168.




